Movement and the Pelvis
A guest blog by Carol Robbins of Alignment Rescue
Carol Robbins is not only a highly respected movement and alignment teacher in her field, she's one of my alignment role models. If you don't have an alignment role model yet, maybe she will be yours as well. Why I love Carol's approach as a Certified Restorative Exercise Specialist (RES) is because it's all about functionally re-training your body so that she can do what she was meant to do: move naturally. This is the foundation upon which everything else is built.
Carol's story has many lessons and advice, but one important message needed for so many endo girls being about modern day fitness - as so often we think we're fit in certain ways only to find out our pelvic floor is shortened and tight (like Carol, even as a pilates instructor, and like yours may be, even if you're a yoga instructor). Or that even though we're technically walking, we're crunching our low sacrum all the while because our legs don't extend behind us like we think. I've received numerous emails from girls with issues such as they can't walk even small distances without back pain, that their uterus is unnaturally tipped or retroverted, and or they have flat feet that make it hard for them to move about their day.
Want to know what these all have in common, and how they relate to your endo pain? Read on, because Carol is a fountain of knowledge.
I suspect many of your readers are young women - the age of my children perhaps (26/29). One of my kids had horrible problems surrounding the menstrual cycle, not diagnosed but no longer an issue as they are non-binary/transitioning. I myself am menopausal. My perimenopausal years were hell, to put it bluntly. I had menorrhagia (abnormal uterine bleeding) that put me in the hospital several times, on the cusp of requiring a transfusion. The doctors had no other advice but to take HRT or birth control pills (I tried the latter, prescribed by the head of gynaecology at the well regarded Women’s Hospital in Toronto. When it didn’t work, I tried to get back in and he was a few months from retiring and refused to see me again - it was several months before I had another doctor).
Eventually I had a D&C and ablation procedure which ended my periods. I didn’t want to start menopause that way, but I had no choice, I was bleeding to death. I had gone through years of tests, biopsies, drug interventions, endless fatigue, hundreds of dollars worth of tampons (until I discovered Diva Cup), 3 or 4 different doctors and was tired of it all.
At the time I was a Pilates teacher and was trying to hide all this from my clients. I would have to run out of a session sometimes two, three times an hour to change my tampon, and it was not just during the duration of a normal period - the bleeding would continue for weeks! It was terribly inconvenient, embarrassing and exhausting.
Fast forward several years and I am no longer a Pilates teacher (or practitioner) but a Nutritious Movement® Certified Restorative Exercise Specialist (RES). My teacher, Katy Bowman, did her masters thesis on the pelvic floor and it’s an area we spend a good deal of time studying.
Of course, pelvic pain is a complex area of study. I am not a medically trained person, but a movement teacher, and I look at the way a person uses their parts most often, how those habits create loads, consider how those loads might affect those tissues (including bones) over the long term. Sitting in a chair creates specific loads to the sacrum and tailbone - both parts of the pelvis - and the fact that we sit so much every day, for most of our lives, has contributed to a culture-wide phenomenon of pelvic dysfunction that is statistically high and getting higher.

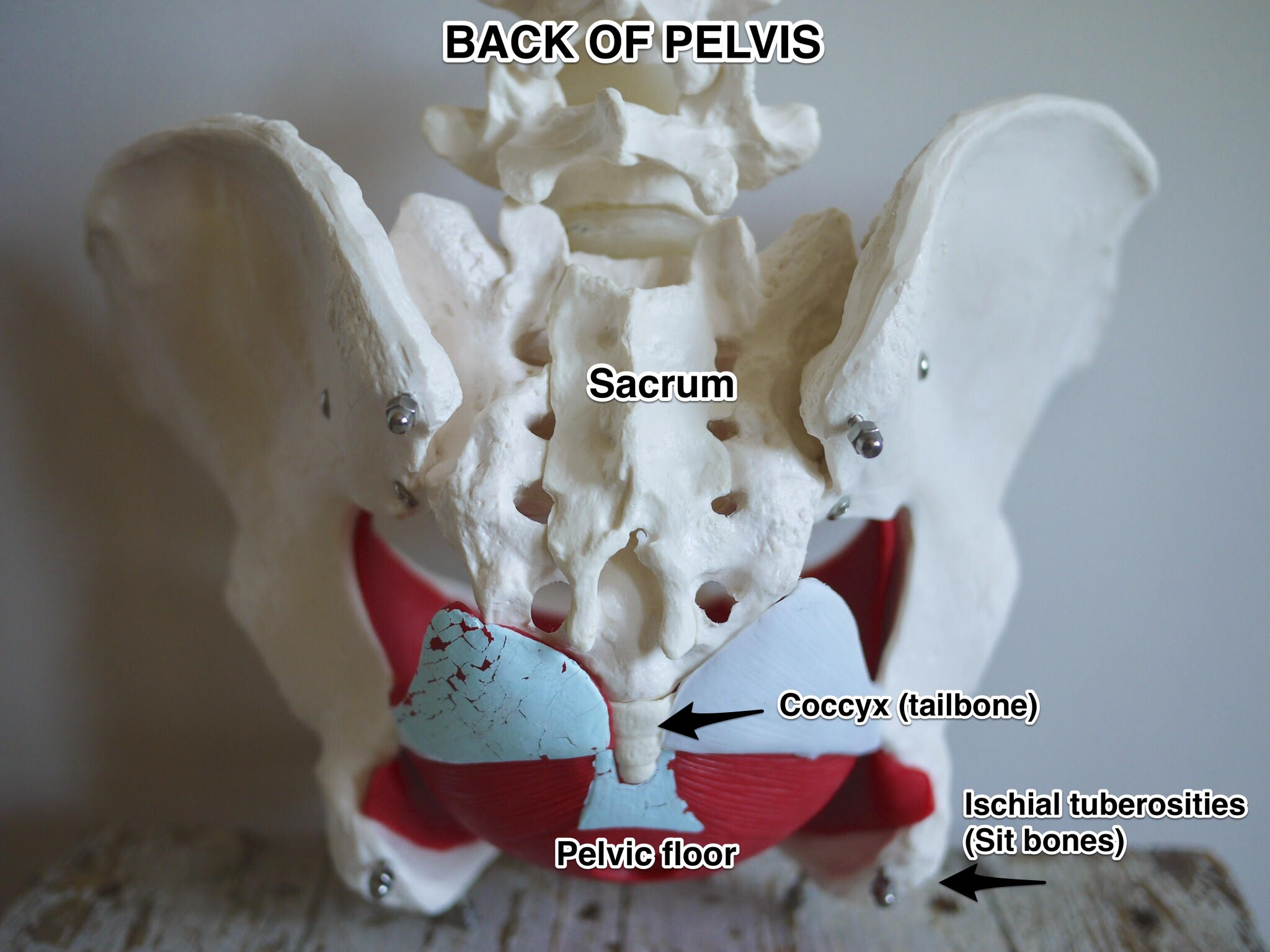
Because the organs in the pelvis are at the positional mercy of their container (i.e your body), how you position your pelvis every day will have an effect on the organs within - they are literally suspended via ligaments from that container. (Sitting also requires little to no pelvic floor participation; the chair supports your pelvis and its contents.) The uterus attaches via the uterosacral ligament to the sacrum. The pelvic floor muscles support from below, but the organ is suspended from this bone, so the position of the sacrum is a very important component to repositioning a tipped uterus, not only by repositioning the pelvis relative to the chair or your standing leg, but also the position of the sacrum relative to the pelvis.
[Heal Endo note: if you just breezed through that paragraph re-read it, because I know most of you girls have a tipped pelvis, which almost always increases endo pain, and very few doctors tell us it's possible to reposition it]
“Our habit of sitting has created hips that can no longer extend, and what often happens instead is the movement to get the leg behind you is transferred to the lower back. Or, the knees bend more than necessary so the foot goes behind you when you walk, but the thigh itself doesn’t.”
The excessive loads that sitting creates is not the only problem, of course, or else our pelvic woes would be easily rectified with standing desks. Here, the pelvis is missing loads as well. It's the act of walking that activates the gluteal muscles which extend the hip (move the leg behind you); muscles which attach to the outside of the sacrum and help create a force on that bone that maintains nutation (the position of the sacrum where the tailbone is moving away from the front of the pelvis, or pubic bone). Nutation gives the pelvic floor its length and resting tension. The reverse (counternutation) moves the tailbone in and shortens the pelvic floor. This is what happens when you sit on the back of the sit bones with the tailbone tucked. So walking is necessary (and a good deal of it), and specifically walking with hips that extend.
Sounds easy. But unfortunately, many people have severely reduced their hip extension range of motion, and some of us are getting from point A to B with no hip extension whatsoever!

no hip extension at all, even though it "looks" like it. Crunch goes the low back, ouch goes the pelvis, weak stay the glutes

this is what proper leg extension looks like - if you can't even get close to this right now don't fret! alignement work takes time and diligence.
Our habit of sitting has created hips that can no longer extend, and what often happens instead is the movement to get the leg behind you is transferred to the lower back. Or, the knees bend more than necessary so the foot goes behind you when you walk, but the thigh itself doesn’t. If you have one of those nifty phones that film in slow motion, have a friend film you walking from the side and have a close look at how much range of motion your hip has and what your knees and lower back are doing. If you have an asymmetrical gait, you’ll have asymmetrical strength on one side of the pelvis (possibly leading to one-sided pelvic issues).

this is me (katie at heal endo) on left when endo was at its worst (see absolutely no leg extension!). on right, 3 years of alignment work later. yup, it takes time.
One of the most commonly prescribed exercises for the pelvic floor is the Kegel, or concentric contraction of the pubococcygeus muscles. If this is done in a situation where the pelvic floor is shortened due to sacral counternutation, the pelvic floor shortens further and can eventually fail (again) after a brief respite. The key is to perform this activity on a lengthened pelvic floor, one which is supported from the other side of the sacrum with robust gluteal activity from frequent hip extension. This stabilizes the sacrum and allows optimal force generation from the PF muscles, which is the whole point right?
One of the simplest things you can do for your pelvic floor isn’t even at the pelvic floor, but way down below it at your feet! One of the pelvic floor muscles attaches to the top of the leg (obturator internus). If you toe out, or duck walk, the position of the foot changes the position of the hip and you cannot attain optimal strength of the pelvic floor muscles. Walking with the feet straighter rotates the head of the femur (hip) and lengthens this muscle. [read the links below for specific examples of how to strengthen your feet!]

Even though I am menopausal now, and it would be easy to coast into my golden years without addressing my PF issues, which were surgically resolved, the fact that I had issues was a red flag (unfortunate pun!) that there were existing underlying problems. I’ve been working at it ever since and although it’s too late to know for certain whether my work would have fanned the pelvic flames during that period (I did it again!), I’ve been delighted to have other issues reduced: I am no longer stress incontinent - no “sneeze pee.” Although I doubt I’ll ever be able to jump on a trampoline (too much force) I can walk and sneeze or laugh at the same time.
What I thought was a lifetime of maintenance and preparation (stop, squeeze the legs together, close my sphincters - ACHOO!) is now a reminder to sneeze up and out and not down. The Restorative Exercises I couldn’t do (even as an advanced Pilates practitioner) are now easy and pleasant. Proximal hamstring pain - gone. (This is an area of pain at the top of the back of your leg where the hamstrings attach to the pelvis.) Hip range of motion increased, including extension, which helps me maintain my gluteal strength just by walking to do my daily chores. There are many other examples of improvement to my health and wellness due to my RE practice that are related to pelvic health as well, such as foot health, breathing function, and abdominal function.
I think regardless of what pelvic health issues you are experiencing, it is worthwhile to have a look at your biomechanics and try to optimize the health of all the pelvic floor and hip muscles and related tissues. When you’re my age, you can thank me.

Carol Robbins is a Toronto based RES-CPT who teaches movement to all ages. She can be found at www.alignmentrescue.com where she maintains a blog, and on Facebook at Instagram as Alignment REScue. She also offers help via Skype. More information and contact information can be found on her website.
Links for Foot Health:
http://www.alignmentrescue.com/lifestyle-tips-to-support-foot-health/
http://www.alignmentrescue.com/foot-mobility-top-of-foot-stretch/
http://www.alignmentrescue.com/anatomy-of-the-top-of-foot-stretch/
http://www.alignmentrescue.com/lifestyle-tips-to-support-lower-leg-health/
http://www.alignmentrescue.com/no-foot-no-horse/
http://www.alignmentrescue.com/ultimate-guide-to-the-bunion/
Pelvic Health:
http://www.alignmentrescue.com/the-gift-of-healthy-bowel-movements/
http://www.alignmentrescue.com/hip-extension-or-spine-extension/
http://www.alignmentrescue.com/feet-and-the-pelvic-floor/
http://www.alignmentrescue.com/clamshells-my-ass/
http://www.alignmentrescue.com/how-to-stretch-your-quads/
I am a Nutritional Therapist, certified though the Nutritional Therapy Association, but I am not a dietitian, doctor, or medical professional, and this site is solely for guidance and information to give people more information to make an informed decision about their own bodies best treatment plan. Please check with your doctor or care provider before making changes in your life