Can Endometriosis Go Away? Reasons for Hope
Endometriosis is a chronic inflammatory disease defined by the growth of abnormal, endometrial-like tissue outside of the uterus. These endometriotic lesions (i.e., endometriosis), grow and bleed in response to hormonal fluctuations throughout the menstrual cycle. This is probably why the endometriosis lesions are so often confused with the endometrium, although they are quite different.
Endometriosis can also be progressive, which means lesions can grow, spread, infiltrate, trigger the creation of scar tissue and adhesions, and lead to worse forms of disease.
All of this together doesn’t set the stage for not much hope, does it!?! I mean, how many of us were told that “there is no cure” or that managing symptoms (over 100’s of them for some of us) will be our forever lot in life? I know I was.
At the same time, you may have read about women who ended up having endometriosis and being just…fine. Perhaps even exceptionally well (like me). Women who “used to have endo,” and now it never rears its ugly head. What gives?
This begs the question, can endometriosis go away?
To fully understand endometriosis behaviors (how it can establish, grow, or shrink), I hope you read my book Heal Endo. For now, I’ll give you a cliff notes answer to this question: Yes, it can. But that “yes” is very, very nuanced. Technically yes, for some lesions, in some people, in some circumstances. On the other hand, lesions can remain although without causing damage or symptoms. Read on.
Can Endometriosis Go Away?
While many endometriosis stories are truly heartbreaking, it’s important to note that endometriosis isn't symptomatic or progressive for all patients. In fact, these following studies, following humans not animals, suggest that lesion stabilization or regression is more common than progression!
A review found while 29% of endometriosis cases showed progression, 42% exhibited disease regression, and 29% remained stable. 71% stabilized or regressed. [1]
Nearly 6% of women getting their tubes tied had asymptomatic endometriosis, which was established but not progressing. If we estimate 10% have endometriosis, and 5% were asymptomatic, we could estimate 60% stabilized/non-problematic. [2]
A study followed women with moderate or severe endometriosis nearly 2 years. Results showed that 37% experienced further nodule development or growth, 13% saw a reduction in nodule number or size, and 50% remained unchanged. 63% stabilized or regressed. [3]
Another study by Fedele et al. tracked untreated asymptomatic rectovaginal endometriosis patients for 1 to 9 years. Only 2% developed symptoms related to endometriosis, 5% saw lesion growth without symptoms, and 93% showed no clinical changes. [4]
Collectively, these studies suggest that endometriosis stabilization or regression rates range from 63% to 93%, while progression rates range from 7% to 37%. That is hopeful.

But there’s more! For some of us, endometriosis may even be prevented before it becomes a problem. How? Once endo-like cells appear within the body, it is the job of your immune system to clean them up. This is what a normally functioning immune system does; it finds abnormal and/or mutated cells and removes them.
This may be why very active microscopic endometriosis lesions have been documented in healthy women, which seem to appear and disappear without progressing to cause pain or damage. That’s right, their bodily processes (correctly functioning) address them promptly before they become an issue. [5]
Similarly, research has shown that while up to 10% of fetuses may be born with endo-like cells in the deep cul-de-sac tissue, less than 4% develop endometriosis here. This means something happened to prevent active endo in 60% of those patients.[6]
This makes a little more sense when we understand where endometriosis comes from: our own bodies. Endometriosis cells are not made from aliens, witches, or a lab in Wuhan that randomly placed these cells inside of you. These are your cells, just epigenetically and genetically altered to behave differently (aggressively in some cases), and living in a place they absolutely should not be. The fact that endometriosis is you mean it’s actually misbehaving bodily processes that got you into this mess in the first place (not aliens or lab leaks).
This is not to say it’s your fault, not at all, more like it’s totally not your fault—it was all a big bodily mistake.
So when the mistaken bodily processes are supported in healing, we may see stabilization or regression. When they are fostered, we can see progression.
How to Support Regression? Meet Salugenesis
But, before you run to your doc yelling “ENDOMETRIOSIS CAN GO AWAY!” know that genetics, epigenetic changes, environmental factors, bacteria, nutritional deficiencies, hormonal imbalances, and more (whoa!) interact uniquely with each patient, making some more susceptible to endometriosis development and progression than others. More simply put: we’re all unique! While some appear to clear lesions before they are established, others may more easily progress. Some of us need an excision surgery more than anything to begin the healing process, others of us will do fine healing without one.
However, by understanding the bodily processes that support progression (endo-ing) and those that support stabilization or regression, we can stack the deck in our favor for better endometriosis outcomes.
To describe how healing like this works, we can use the word salugenesis, coined by respected researcher Dr. Naviaux. Salugenesis is the creation or support of cellular healing, a word used in opposition to pathogenesis, the creation of disease. He writes: “Salugens are interventions that promote the completion of the healing cycle, restore health, decrease mortality, and create heightened states of health and resilience.” [7]
If antibiotics are what heal acute infections, salugens are what heal chronic diseases (which are much, much more complex and multifactorial than an infection).
Salugens can be anything that promotes the healing of tissues and cells. Getting rid of a chronic bacterial or viral trigger is salugenic; removing chemical or toxin exposure, reversing essential nutrient deficiencies, regulating the nervous system and increasing vagal tone, sleeping well, adaptogens, and physical therapy can all be salugenic. Surgical removal of endometriosis lesions is salugenic. Everything I write about in Heal Endo can be deemed salugenic. [Also, why it’s important not to get caught up on one single healing modality alone, like a diet! There are so many factors at play here, my friends.]

Endometriosis Healing Relies on Whole Body Healing
In my book, I refer to this concept as the healing of a whole-body ecology. Ecology itself is the scientific study of the interconnected relationship between living organisms and their environment. For example, when studying the ecology of a forest, a tree is as important to understand as a leopard, bug, grass, rainfall, and even wind pattern. Each contributes to the proper health of that environment. Using this example, we can use the term “whole-body ecology” to describe the same type of interwoven relationship between the eleven main systems within their environment, the human body:
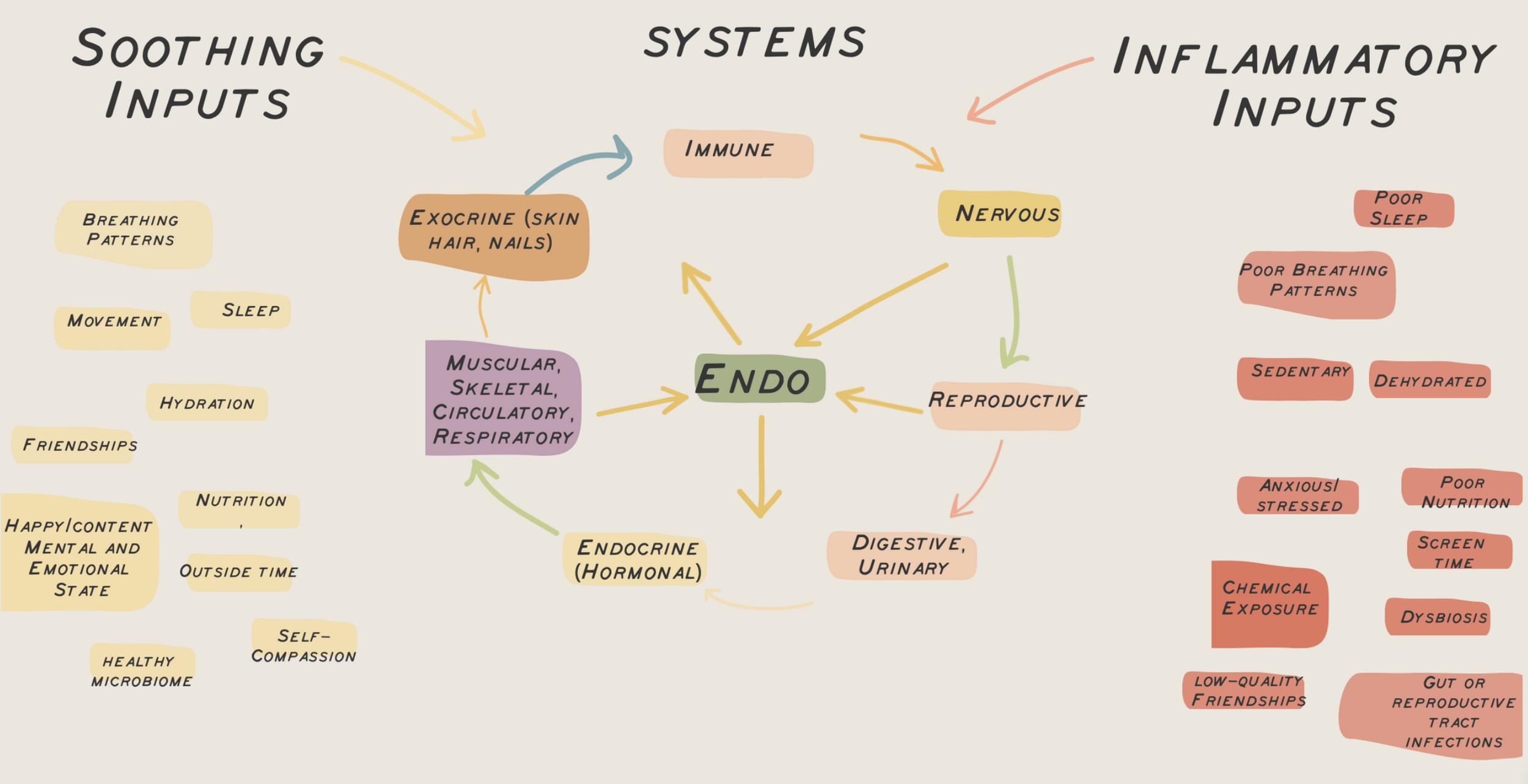
To properly function, these systems all rely on a continuous stream of healthy, soothing inputs. This includes proper nutrition, hydration, a calm and loving mental/emotional state, proper breathing patterns, adequate sleep, few toxins, and so much more. When most inputs are beneficial like this, these systems will communicate properly, working in harmony to maintain balance in the body. Cells and tissues can heal.
The problem begins when modern-day living slaps our body ecology with so many negative inputs that our systems respond in more problematic than beneficial ways.
Too much battery will start to create dysfunction within these systems and the communication between them. What emerges is an inflammatory body ecology that benefits endometriosis—development, progression, or even just symptoms. It’s how pathogenic bacteria from the digestive or reproductive tract may stimulate lesions to grow, while removing bacterial overgrowths may support the regression of lesions; how nutrient deficiencies may foster endo progression, whereas nutrient infusion may help curtail disease; how high levels of stress hormones may increase lesion size and volume, whereas the elimination of stress hormones may prevent endometriosis recurrence.
This is why diet, lifestyle, and complementary methods that support whole-body health are essential considerations when healing from endo.
That’s because, in a very generalist view, endometriosis regression lies in the ability of your cells to heal, a sophisticated process of immune factors, nervous system communication, hormone communication, safety from damaging triggers, and more for tissues to mend. By understanding the inputs that support whole body healing, we can do our best to stack the deck in our favor.
PSA: This Information Doesn’t Make Light of Endometriosis!
There are a lot of patients who have suffered immensely from endometriosis: physically and psychologically. I’ve heard (and experienced) insane stories of medical negligence, normalization of life-altering symptoms, patient care, community support, and more. So please know that this information about endo being able to stabilize or regress is not making light of a disease that can 100% wreck lives.
Nor should this information EVER be used to inform people their endo can “simply” go away on its own, their symptoms aren’t real, or that surgery or drug therapies aren’t warranted. We are all unique, and the complexities of this disease, combined with the unique immune, hormonal, nervous system, and bacterial “footprint” of each sufferer, make it impossible to create a roadmap to remission that works for all.
In fact, when it comes to body ecology, once endometriosis lesions are established, they don’t just respond to body ecology but actually start contributing to the equation. It’s one reason why endometriosis is considered a full-body disease, both impacting and being impacted by a whole-body ecology gone rogue. It’s also why surgical removal of endo lesions and subsequent damage by an endo specialist surgeon is an important step to consider.
Moreover, endometriosis lesion size is not directly correlated with endometriosis symptom intensity. You can have small lesions or stabilized lesions causing pain, while you can have progressive lesions causing no symptoms at all. This is why addressing endometriosis has a two-pronged goal: preventing damage/progression and reducing symptoms.
This is also why surgical removal of lesions is super important for many, especially those whose endometriosis does not appear to stabilize or regress, those with continual systemic issues (MCAS, chronic fatigue, recurrent infections, etc), and those whose quality of life does not improve.
For this post we’re just chatting lesion behavior :)
Back to Endometriosis Healing Hope
Those important points aside, I want this information to offer magical levels of hope for the many patients who have been told, “You will never heal.” And the patient journey is what I’m here in the space to support most!
The hope here is knowing that endometriosis lesions
a) Can stabilize or regress, thanks to your bodily processes “cleaning them up”
b) Can continue to exist without causing damage or progressing, existing in a place of “remission”
Even more exciting, we know many facets to help get here. Some of the biggest ones in the holistic healing world are:

Medical salugens are important too!
Early diagnosis should be mandatory, not optional, since this sets the stage for healing before more complexities arise. Preventing progression is crucial to preserve fertility and avoid irreversible tissue damage.
Eradicating underlying infections such as SIBO, dysbiotic patterns, or reproductive tract dysbiosis.
Considering the use of oral contraceptives or other hormonal medications to help
So while this is a bit of a high level post (sorry!), I hope it brings hope and a newfound understanding of how endometriosis behaves. I believe hope is a necessary ingredient to maintain in our fight back to good health, and understanding that endometriosis is not always progressive is a great place to start.
In health,
Katie
The information provided on Heal Endo is for general informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or another qualified health provider with any questions you may have regarding a medical condition.
1) Evers, J.L.H. (2013). Is adolescent endometriosis a progressive disease that needs to be diagnosed and treated? Human Reproduction, 28(8), 2023. https://doi.org/10.1093/humrep/det298
2) To note, because of the normalization of pain, it’s possible these women had symptoms to some degree but considered it normal. Fuentes, A, Escalona, J, Céspedes, P, Espinoza, A, Johnson, MC. (2014). Prevalencia de la endometriosis en mujeres sometidas a esterilización quirúrgica laparoscópica en un hospital de Santiago de Chile [Prevalence of endometriosis in 287 women undergoing surgical sterilization in Santiago Chile]. Rev Med Chil, 142(1), 16-19. Spanish. https://doi.org/10.4067/S0034-98872014000100003
3) Knez J, Bean E, Nijjar S, Tellum T, Chaggar P, Jurkovic D. Natural progression of deep pelvic endometriosis in women who opt for expectant management. Acta Obstet Gynecol Scand. 2023 May 15. doi: 10.1111/aogs.14491.
4) Fedele L, Bianchi S, Zanconato G, Raffaelli R, Berlanda N. Is rectovaginal endometriosis a progressive disease? Am J Obstet Gynecol 2004b, 191:1539-1542. doi: 10.1016/j.ajog.2004.06.104. PMID: 15547522
5) Koninckx, P. R., Donnez, J., & Brosens, I. (2016). Microscopic endometriosis: impact on our understanding of the disease and its surgery. Fertility and Sterility, 105(2), 305–306. https://doi.org/10.1016/j.fertnstert.2015.10.038
6) Signorile, P. G., Baldi, F., Bussani, R., D'Armiento, M., De Falco, M., & Baldi, A. (2009). Ectopic endometrium in human foetuses is a common event and sustains the theory of müllerianosis in the pathogenesis of endometriosis, a disease that predisposes to cancer. Journal of Experimental & Clinical Cancer Research: CR, 28(1), 49. https://doi.org/10.1186/1756-9966-28-49; Koninckx, P. R., & Martin, D. C. (1992). Deep endometriosis: a consequence of infiltration or retraction or possibly adenomyosis externa?. Fertility and Sterility, 58(5), 924–928. https://doi.org/10.1016/s0015-0282(16)55436-3; Martin DC; Koninckx PR; Batt RE; Smith R. “Deep endometriosis” in Minaguchi, H; Sugimoto, O (eds). Endometriosis Today: Advances in Research and Practice. Lancaster, Parthenon Publishing Group. pp. 50-57, 1997
7) Naviaux R. K. (2023). Mitochondrial and metabolic features of salugenesis and the healing cycle. Mitochondrion, 70, 131–163. https://doi.org/10.1016/j.mito.2023.04.003